










English
M-5276-559C 7
fluoroscopy and electrograms to aid in proper positioning.
9.
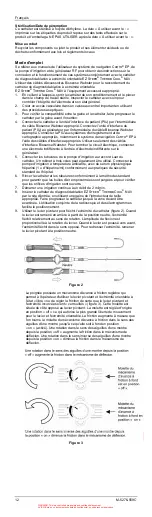
Use the Rocker Lever to deflect the catheter tip (Figure 2). When the lever
is pulled back from neutral, the tip will deflect relative to the direction of
rotation. The amount of deflection is relative to the amount of lever
rotation. When the lever is pushed forward, the tip will deflect in the
opposite direction. To straighten the tip, return the Rocker Lever to neutral
position.
Figure 2
The handle has an adjustable friction control that allows the operator to
use the Rocker Lever and deflecting tip in a “free” state or adjust the
friction to where the Rocker Lever and tip curve are “locked” in place
(Figure 3). This knob is located on the opposite side of the Rocker Lever.
Out of the package, the knob will be in the “off” position, which allows the
freest movement for the lever and deflecting tip. The amount of friction
increases as the Friction Control Knob is rotated clockwise until it reaches
the fully “on” position. Clockwise rotation from the “off” position increases
the friction within the Deflection Mechanism. Counter-Clockwise rotation
from the “on” position decreases the friction within the Deflection
Mechanism.
Figure 3
10.
For RF application and flow settings refer to Table 1
Table 1: RF and Flow Settings
RECOMMENDED RF APPLICATION PARAMETERS
ATRIAL
ABLATION
VENTRICULAR
ABLATION
Power Range
15 W to 30 W*
31 W to 50 W
Temperature Monitoring
<50°C**
<50°C**
Irrigation Flow Rate During
RF Application
17 ml/min
30 ml/min
Application Time
30 to 120 seconds
60 to 120 seconds
* Power levels exceeding 30 Watts may be used when transmural lesions
cannot be achieved at lower energy levels. For power settings > 30 Watts,
the recommended irrigation flow rate is 30 ml/min.
** The temperature displayed on the RF generator does not represent tissue
temperature or electrode tissue interface temperature.
Additional recommendation:
For isthmus dependent flutter ablation, power applications exceeding
30 watts and up to 50 watts should only be used if conduction block cannot
be achieved at lower power levels.
11.
Recommendation for irrigation: Increase the irrigation to high flow rate
starting up to 5 seconds before the onset of RF energy delivery and
maintaining this higher flow rate until 5 seconds after termination of the
energy application. For power levels up to 30 watts, a high flow rate of
17ml/min should be used. For power levels between 31-50 watts, a high
flow rate of 30ml/min should be used.
12.
The application of RF energy must not be initiated until the increase in
irrigation flow rate is confirmed by a minimum of 2º C decrease in tip
electrode temperature.
13.
Monitor the catheter tip temperature throughout the procedure to ensure
adequate irrigation. The peak temperature should not exceed 50
o
C during
RF energy delivery. Note: the displayed temperature represents the
temperature of the electrode only, not the temperature of the tissue.
14.
Start a procedure at 15-20 Watts. After 15 seconds, power may be
increased by 5-10 W increments as needed, until a transmural lesion is
achieved. The duration of each RF ablation should not exceed 120
seconds. Dragging the catheter to the next location is permissible during
the 120-second energy application.
15.
RF current may be reapplied to the same or alternate sites using the
same catheter. However, in the event of a generator cutoff (impedance or
temperature), the catheter must be withdrawn and the tip electrode
inspected for coagulum before RF current is reapplied. To remove any
coagulum, if present, a sterile gauze pad dampened with sterile saline
may be used to gently wipe the tip section clean; do not scrub or twist the
tip electrode as damage to the tip electrode bond may occur and loosen
the tip electrode. Prior to reinsertion, ensure that the irrigation holes are
not plugged by increasing the flow rate and verifying flow from each of the
six irrigation holes.
If irrigation hole occlusion occurs:
a) Fill a 1 or 2 ml syringe* with sterile saline and attach to the stopcock
or sidearm.
b) Carefully inject the saline from the syringe into the catheter. A stream
of fluid should be visible from all six (6) holes.
c) Repeat steps a and b, if necessary until the holes are cleared.
d) Flush catheter and tubing per standard technique to ensure purging
of trapped air bubbles and to verify that the irrigation holes are patent.
e) The catheter can now be introduced into the patient.
WARNING: This is a controlled proprietary and confidential document.
AVISO: Este es un documento controlado, confidencial, y con derechos reservados.