10
3.0. Product use
3.1. Preparation before use
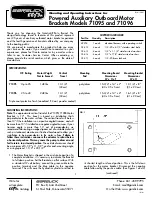
SIZE SELECTION
Ambu Aura-i comes in different sizes for use in patients of
different weights.
For pediatric patients, it is recommended that Ambu
Aura-i is used by a medical professional familiar with
pediatric anesthesia.
See selection guidelines and max. intracuff pressure in
Table 1, section 4.0. (Specifications).
INSPECTION OF AURA-I
Always wear gloves during the preparation and insertion of
Ambu Aura-i to minimize contamination.
Handle Aura-i carefully as it can be torn or punctured.
Avoid contact with sharp or pointed objects.
Check that the pouch seal is intact before opening and
discard Ambu Aura-i if the pouch seal has been damaged.
Closely examine Aura-i for any damage, such as perforation,
scratches, cuts, tears, loose parts, sharp edges etc.
Make sure that the cuff protector has been removed from
the cuff.
Check that the interior of the patient tube and the cuff are
free from blockage and any loose parts. Do not use Aura-i
if it is blocked or damaged.
Deflate the cuff of Aura-i completely. Once deflated, check
the cuff thoroughly for any wrinkles or folds. Inflate the cuff
to the volume as specified in Table 1. Check that the inflated
cuff is symmetrical and smooth. There should not be any
bulge nor any sign of leakage in the cuff, pilot tubing or
pilot balloon. Deflate the cuff again before insertion.
3.2. Preparations for use
PRE-INSERTION PREPARATION
• Deflate the cuff completely so that the cuff is flat and
free of wrinkles by pressing the cuff down onto a flat
sterile surface (e.g., a piece of sterile gauze) while at the
same time deflating the device with a syringe.
3
• Lubricate the posterior tip of the cuff prior to insertion
by applying a sterile, water-based lubricant to the distal
posterior surface of the cuff.
• Always have a spare Ambu Aura-i ready for use.
• Pre-oxygenate and use standard monitoring procedures.
• Check that the level of anesthesia (or unconsciousness)
is adequate before attempting insertion. The insertion
should be successful at the same level of anesthesia
that would be suitable for tracheal intubation.
• The head of the patient should be positioned extended
with flexion of the neck in a position normally used for
tracheal intubation (i.e., “the sniffing position”).
3.3. Insertion
• Never use excessive force.
• Hold the connector shell with the thumb on the vertical
line on the connector shell and three fingers placed
on the opposite side of the connector shell. Your other
hand should be placed under the patient’s head.
4
• Insert the tip of the cuff pressing upwards against the
hard palate and flatten the cuff against it.
5
• Verify that the tip of the cuff is flattened against
the palate before proceeding – push the jaw gently
downwards with your middle finger to open
the mouth further.
• Ensure that the tip of the cuff avoids entering the
valleculae or the glottic opening and does not become
caught up against the epiglottis or the arytenoids. The
cuff should be pressed against the patient’s posterior
pharyngeal wall.
• When the mask is in place, resistance will be felt.
• After insertion ensure lips are not trapped between
connector shell and teeth to avoid trauma to lips.
INSERTION PROBLEMS
• For pediatric patients, a partial rotational technique is
recommended in case of placement difficulties.
• Coughing and breath-holding during Ambu Aura-i
insertion indicates inadequate depth of anesthesia –
Immediately deepen anesthesia with inhalational or
intravenous agents and initiate manual ventilation.