

























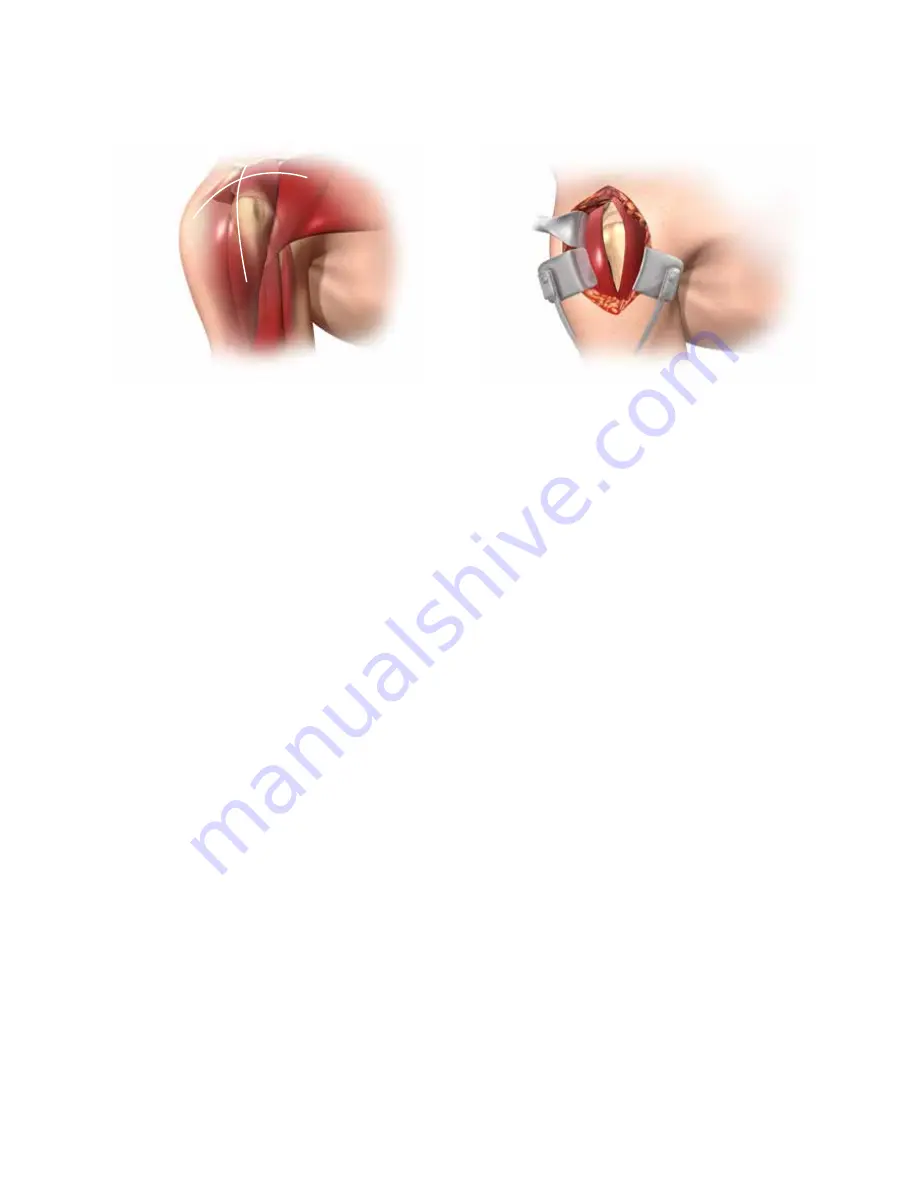
Figure 4
Figure 5
11
10
extend more than 4 cm from the external aspect of the
acromion in order to preserve the axillary nerve which is
located below the turning fold of the subacromial bursa.
17
When the subacromial bursa is visible, gentle longitudinal
traction in line with the limb allows a retractor to be
placed in the subacromial space. The anterior deltoid is
then released subperiostally from its acromial insertion
up to the Ac joint. The deltoid release from the anterior
acromion can include a small piece of bone to facilitate
repair and to protect the deltoid muscle.
once the subacromial bursa has been removed, the
humeral head is visible at the anterior edge of the
acromion. Exposure may be improved, if necessary, by
dividing the Ac ligament and performing acromioplasty.
The limb is then externally rotated and the head is
dislocated antero-superiorly to facilitate positioning of the
cutting guide. if the bicep is still present, a tenotomy or
tenodesis should be performed. The subscapularis, teres
minor and infraspinatus are retained when present. A
partial detachment of the subscapularis may be performed
when the superior dislocation of the humerus is difficult
to obtain.
suRgicAL AppRoAch: supERioR-LATERAL
The DELTA XTEND Reverse shoulder system prosthesis
can be implanted using a superior-lateral deltoid split
approach or a delto-pectoral approach. The choice
depends on the surgeon’s preference and clinical
parameters.
The delto-pectoral approach has the advantage of offering
an enhanced view of the inferior part of the glenoid.
Revision surgery is usually performed using a delto-
pectoral approach so the approach can be made through
the original scar and it allows for a longer humeral incision
when faced with difficult removal of the humeral stem.
Alternatively, the superior-lateral approach enables clear
visualisation of the glenoid and therefore facilitates the
implantation of the glenoid components of the prosthesis,
in particular where the glenoid is retroverted. moreover,
this approach does not necessitate the partial detachment
of the subscapularis muscle that could be seen as further
weakening of the remaining cuff structure.
Superior-lateral Approach
The skin incision is 10-12 cm and can be antero-posterior
along the lateral edge of the acromion or made in a lateral
direction (Figure 4). Following subcutaneous dissection,
separate the anterior and middle deltoid muscle bundles
opposite the lateral margin of the acromion using blunt
dissection (Figure 5).
The dissection starts at the level of the Ac joint, 5-7 mm
posterior to the tip of the acromion and extends straight
laterally down into the deltoid muscle. it should not







































































