www.bedfont.com
11
NOxBOX
®
mobile Operating Manual
English
Initial Purge
IMPORTANT: Residual NO gas left in the
system may convert to NO
2
during storage. This
purge procedure MUST be followed prior to use
on a patient to ensure that any residual gas from
previous use has been flushed out.
SAFETY: Refer to all safety notices regarding
handling the gas and using suitable ventilation
to prevent build-up of unsafe atmospheres.
During purge, the exhaust from the unit should
be fed through an appropriate atmospheric
scrubber or a scrubber filter for NOx gases.
This will safely remove the toxic nitrogen oxides
from the gas exhaust. Contact Bedfont or your
distributor for NOx scrubber information.
NOTICE: If system is left pressurised following
purge for more than 4 hours without use, this
purge procedure must be repeated to ensure
safe application.
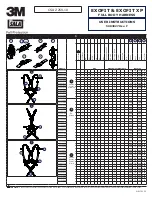
● Ensure the Changeover Dial (See Fig.5,
item B) arrow is pointing to cylinder 1. Turn
on cylinder 1 by opening the cylinder valve
carefully.
● The Pressure 1 gauge dial should register
the contents pressure of the cylinder (See
Fig. 5, item A). Ensure there is sufficient
pressure in the cylinder to commence
treatment. A full cylinder is approximately
150 - 200 bar (check with your supplier). A
cylinder is “empty” at 10 bar.
● The outlet pressure gauge dial (Fig. 5, item
E) should read 2 bar.
● Open the valve on the flow meter (Fig. 5,
item G) until the flow reads approximately
600 cc/min. IMPORTANT: do not open valve
beyond maximum flow indicated on the flow
meter (Fig. 3, item H) as this may damage
the instrument control.
● Allow the system to purge for 10 minutes
before switching off cylinder 1 at the cylinder
valve. Do not over-tighten the cylinder valve
when closing.
● Repeat this purge procedure for cylinder 2.
● Close the valve on cylinder 2 and carefully
close-off the flow meter. NOTE: when fully
closing the valve, be careful to not over-
tighten as this may cause damage to the
control valve mechanism.
● Ensure both cylinder valves are shut off
by end of the purge procedure and prior to
connecting to patient.
Figure 5