







• 2 •
Insertion Instructions
1. Identify the Vein and Insertion Site
A. Apply a tourniquet above the anticipated insertion site.
B. Select a vein by assessing patient anatomy and condition. Recommended veins are cephalic,
basilic or median cubital basilic.
Caution: The PowerPICC SOLO*2 catheter features a
reverse-taper catheter design. Placement of larger catheters at or below antecubital fossa
may result in an increased incidence of phlebitis. Placement of
PowerPICC SOLO*2 catheter
above antecubital fossa is recommended.
C. Release tourniquet.
D. Set up the sterile field.
2. Preflush the Catheter and Stylet
A. Flush the catheter with heparinized saline solution or sterile
normal saline.
Note: The catheter may be trimmed if a
shorter length is required.
Optional: For use only when the catheter is not inserted using the over the wire insertion technique.
B. Attach a syringe with sterile normal saline to the Luer Lock fitting of the flush through stylet
hub.
C. Inject enough solution to wet the stylet surface entirely. This will activate the hydrophyllic
coating, making the stylet surface very lubricious.
D. Remove the stylet from its holder and insert it into the catheter. If the catheter has been
trimmed, only advance the stylet to the distal end of the catheter.
Note: If the surface of the
stylet becomes dry after removal from the holder, wetting with additional sterile normal saline
will renew the hydrophyllic effect.
E. The catheter stylet assembly can now be introduced as described in the following information.
3. Apply Tourniquet and Drape
A. Position arm at 90° angle.
B. Re-apply the tourniquet above the intended insertion site to distend the vessel.
C. Prepare the site according to institution policy using sterile technique.
D. Drape the patient by placing the fenestrated drape over the anticipated puncture site.
E. When alcohol is used as a skin prep, it must be allowed to completely air dry.
4. Perform Venipuncture
A. Remove the needle guard and attach a syringe.
B. Introduce the needle into the vessel and observe for flashback.
C. When the vein has been entered, remove the syringe leaving
the needle in place.
WARNING: Place a finger over the orifice of the sheath to
minimize blood loss and risk of air aspiration. The risk of air
embolism is reduced by performing this part of the procedure
with the patient performing the Valsalva maneuver until the
catheter is inserted into the sheath.
Caution: Avoid placement or securement of the catheter
where kinking may occur, to minimize stress on the catheter, patency problems or patient
discomfort.
Caution: The PowerPICC SOLO*2 catheter features a reverse-taper catheter
design. Placement of larger catheters at or below antecubital fossa may result in an increased
incidence of phlebitis. Placement of the
PowerPICC SOLO*2 catheter above antecubital fossa
is recommended.
5. Advance Guidewire
A. Introduce the guidewire through the needle; advance the
guidewire 15 to 20 cm into the vessel.
Caution: Do not advance
the wire past the axilla without fluoroscopic guidance or other tip
locating methods.
6. Remove Needle
A. Release tourniquet. Apply slight pressure on the vessel above
the insertion site to minimize blood flow.
B. If necessary, enlarge the puncture site with a #11 scalpel blade.
C. Leaving the guidewire in place, withdraw the needle.
7. Introduce Microintroducer
A. Introduce the microintroducer assembly over the guidewire.
Using a twisting motion, advance the assembly into the
vessel.
8. Measure Distance to Tip Location
A. Using fluoroscopic control, determine the correct catheter length by
advancing the guidewire to the desired catheter tip location in the SVC.
B. Once the guidewire tip is in proper position, mark the length by
clamping forceps onto the guidewire at the skin site.
9. Removing Dilator and Guidewire
A. Rotate locking collar of dilator and remove dilator from sheath.
B. Withdraw the dilator and guidewire, leaving the small sheath in
place.
WARNING: Place a finger over the sheath opening to minimize
blood loss and risk of air aspiration. The risk of air embolism is
reduced by performing this part of the procedure with the patient
performing the Valsalva maneuver until the catheter is inserted into
the sheath.
10. Modification of Catheter Length
Note: Catheters can be cut to length if a different length is desired due to patient size and desired
point of insertion according to hospital protocol. Catheter depth markings are in centimeters.
A. Measure the distance from the insertion site (zero mark) to the desired tip location.
B. Using the guidewire to indicate desired length, retract the stylet behind the point the catheter is
to be cut (if applicable).
C. Using a sterile scalpel or scissors, carefully cut the catheter according to institutional policy if
necessary.
Caution: Do not cut stylet.
D. Inspect cut surface to assure there is no loose material.
E. Re-advance the stylet to the distal end of the trimmed catheter (if applicable).
11. Insert and Advance the Catheter
A. Insert the catheter (and stylet, if applicable) into the microintroducer
sheath.
B. Advance the catheter slowly.
C. Stabilize the catheter position by applying pressure to the vein distal to
the microintroducer sheath.
D. Withdraw the microintroducer sheath from the vein and away from
the site.
E. Split the microintroducer sheath and peel it away from the catheter.
12. Complete Catheter Insertion
A. Continue to advance the catheter. For central placement, when the
tip has advanced to the shoulder, have the patient turn head (chin
on shoulder) toward the insertion side to prevent possible cannulation into the jugular vein.
Caution: The PowerPICC SOLO*2 catheter features a reverse-taper catheter design.
Placement of larger catheters at or below antecubital fossa may result in an increased
incidence of phlebitis. Placement of the
PowerPICC SOLO*2 catheter above antecubital fossa
is recommended.
B. Position the arm at a 90° angle, maintaining sterility. Complete
catheter advancement into the desired position (zero mark).
WARNING: This is not a right atrium catheter. Avoid positioning
the catheter tip in the right atrium. Placement or migration of the
catheter tip into the right atrium may cause cardiac arrhythmia,
myocardial erosion or cardiac tamponade. The risk of these
complications may be more likely in neonatal patients.
C. Stabilize the catheter position by applying light pressure to the vein
distal to the insertion site. Slowly remove the stylet, if applicable
D. Place a finger over the catheter opening to minimize blood loss.
13. Aspirate and Flush
A. Attach primed extension set and/or saline-filled syringe.
B. Aspirate for adequate blood return and flush catheter with 10 ml normal saline to ensure
patency.
Caution: The PowerPICC SOLO*2 catheter is designed for use with needleless injection caps
or “direct-to-hub” connection technique. Apply a sterile end cap on the catheter hub to prevent
contamination when not in use.
Use of a needle longer than 1.6 cm may cause damage to
the valve. Caution: Always remove needles or syringes slowly while injecting the last 0.5 ml
of saline.
C. Cap catheter.
WARNING: The fluid level in the catheter will drop if the catheter connector is held above the
level of the patient’s heart and opened to air. To help prevent a drop in the fluid level (allowing
air entry) while changing injection caps, hold the connector below the level of the patient’s
heart before removing the injection cap.
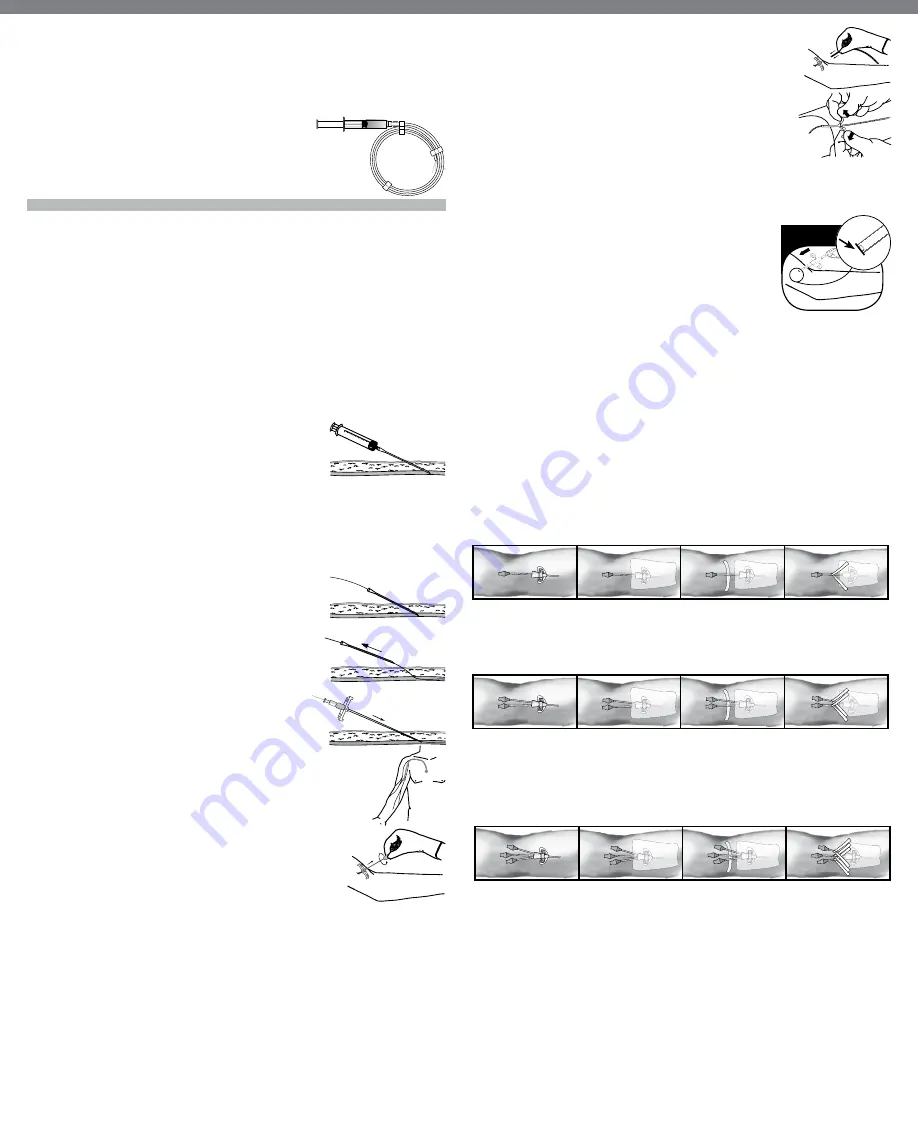
14. Dress Catheter
StatLock* Catheter Stabilization Device Procedure
Single Lumen
1. Secure catheter with
StatLock* catheter stabilization device.
2. Cover site and
StatLock* catheter stabilization device with transparent dressing.
3. Place anchor tape sticky side up, under hub. Wedge tape between hub and wings.
4. Chevron anchor tape on top of transparent dressing.
Dual Lumen
1. Secure catheter with
StatLock* catheter stabilization device.
2. Cover site and
StatLock* catheter stabilization device with transparent dressing.
3. Place 1st anchor tape sticky side up, under one extension leg. Wedge tape between hub and wings.
Chevron anchor tape on top of transparent dressing.
4. Place 2nd anchor tape sticky side up under hub. Wedge tape between hub and wings. Chevron anchor
tape on top of transparent dressing.
Triple Lumen
1. Secure catheter with
StatLock* catheter stabilization device.
2. Cover site and
StatLock* catheter stabilization device with transparent dressing.
3. Place 1st anchor tape sticky side up, under one extension leg. Wedge tape between hub and
wings. Chevron anchor tape on top of transparent dressing.
4. Place 2nd and 3rd anchor tapes sticky side up under remaining hubs. Wedge tape between hubs
and wings. Chevron anchor tape on top of transparent dressing.
3
4
5
6
7
8
9
10
11
12
0
0
Zero mark