CO O K M E D I CA L I N CO R P O R AT E D
P.O. Box 4195, Bloomington, IN 47402-4195 U.S.A.
Phone: 812.339.2235, Toll Free: 800.457.4500, Toll Free Fax: 800.554.8335
CO O K ( CA N A DA ) I N C .
111 Sandiford Drive, Stouffville, Ontario, L4A 7X5 CANADA
Phone: 905.640.7110, Toll Free: 800.668.0300
W I L L I A M A . CO O K AU ST R A L I A PTY. LT D.
Brisbane Technology Park, 12 Electronics Street, Eight Mile Plains
Brisbane, QLD 4113 AUSTRALIA, Phone: +61 7 38 41 11 88
W I L L I A M CO O K E U R O P E A p S
Sandet 6, DK-4632, Bjaeverskov, DENMARK, Phone: +45 56 86 86 86
©
COOK 2008
PI-BM-BNFMP-EN-200807
AO RT I C I N T E RV E N T I O N
CA R D I O LO GY
C R I T I CA L CA R E
E N D O S CO PY
P E R I P H E R A L I N T E RV E N T I O N
S U R G E RY
U R O LO GY
WO M E N ’ S H E A LT H
www.cookmedical.com
SUGGESTED INSTRUCTIONS FOR FEMORAL PLACEMENT
SUGGESTED INSTRUCTIONS FOR FEMORAL PLACEMENT
1. Introduce fi lter/sheath assembly
Insert the fi lter catheter into the introducer
sheath and
Luer lock
it into position. The
tip of the fi lter catheter will then extend
approximately 1.5 cm beyond the tip of the
sheath. While performing hand injections of
contrast medium through the fi lter catheter
sidearm, the fi lter catheter/introducer sheath
assembly can be properly positioned to initi-
ate fi l ter placement.
When using a femoral
approach, position the fi lter catheter tip just
below (caudad to) the renal veins.
2. Pull fi lter/sheath
Loosen the Tuohy-Borst valve and, while hold-
ing the wire guide pusher stationary, withdraw
the fi lter catheter/introducer sheath assembly
to the mark on the wire guide pusher. This
movement will expose the distal anchoring
hooks. Fluoroscopically, this corresponds to
the position of the junction point of the hook
wires remaining just within the tip of the fi lter
catheter. If this can be clearly visualized with
fl uoroscopy, the mark can be ignored.
NOTE
: At the end of the fi lter, the V-shaped
hook wire struts are readily visible, but fi lter wires
are too fi ne to be identifi ed fl uoroscopically.
3. Anchor hooks
Gently
advance the fi lter catheter/introducer
sheath assembly one time, 1-3 mm, to secure
the hooks to the vena cava wall.
Be certain junction point of distal pair of hooks
is in catheter tip when positioning these hooks
into caval wall. If there is uncertainty regarding
hook fi xation, the catheter may be advanced
up over the hook wires to the edge of the hooks.
The catheter may then be repositioned, and
the fi lter placement re-initiated in a slightly
different caval orientation or level.
CAUTION: Overly forceful or multiple jabs
with the fi lter catheter/introducer sheath
assembly could result in perforation of the
wall of the inferior vena cava by the exposed
hooks and struts of the fi lter.
4. Pull fi lter/sheath
Again, hold the wire guide pusher stationary
and withdraw the fi lter catheter/introducer
sheath assembly 1-3 cm. This will facilitate
subsequent passage of the fi lter wires through
the tip of the fi lter catheter and provide room
for fi lter formation within the vena cava.
CAUTION: Do not withdraw the fi lter catheter/
introducer sheath assembly into the iliac vein.
Repositioning into the inferior vena cava may
prove diffi cult.
5. Push fi lter wires
Holding the fi lter catheter/introducer sheath
assembly stationary and with fl uoroscopic
control, advance the wire guide pusher with
a steady, smooth motion until the junction
point of the proximal hook wires is seen
fl uoroscopically at the fi lter catheter tip.
CAUTION: Do not advance too quickly or
forcefully as wire kinking within fi lter catheter
may occur, making advance ment diffi cult.
Mark
6. Push fi lter/sheath assembly
Advance the fi lter catheter/introducer sheath
assembly so that the proximal junction point
is in close proximity to or overlaps the junction
point of previously positioned hook wires.
NOTE: The approximation or slight overlap
of the junction points ensures adequate
compression and formation of the fi lter wires
and places the second pair of hooks in the
inferior vena cava. Placement of a hook in a
renal vein, or passage of fi lter wires distal to
the fi rst hook position (wire prolapse), may
occasionally occur and is of no consequence.
7. Pull sheath
While maintaining slight forward pressure
on the wire guide pusher, slowly withdraw
the fi lter catheter/introducer sheath assembly.
This will permit the proximal hook wires
to exit the catheter, springing open to
engage with the caval wall. This is readily
seen fl uoroscopically.
To be sure the hooks are completely free
from the fi lter catheter tip, the fi lter catheter/
introducer sheath assembly should be
withdrawn to within approximately 1 cm of
the Bird’s Nest Filter handle attached to the
wire guide pusher.
CAUTION: Do not advance the wire guide
pusher after the proximal hook wires have
exited the fi lter catheter tip. Forceful
advancement of wire guide pusher may
alter the orientation of the fi lter attachment
site, making disengagement diffi cult.
Refer to Suggested Instructions For Use for indications, warnings and precautions.
8. Anchor hooks
Gently tug or use a slight to-and-fro motion
on the wire guide pusher to secure the
second pair of hooks to the vena cava wall
before disengaging the fi lter.
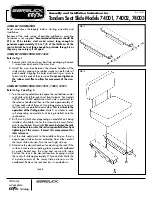
9. Detach fi lter
To release fi lter:
a
. Maintaining wire guide pusher position,
remove red safety lock from handle by
grasping both sides and pulling up and
away from the handle.
b
. Holding the wire guide pusher steady,
use the handle to fully depress the
thumb grip of the wire guide pusher
forward into the cannula. Maintaining
this position will release the fi lter.
Separation can be seen fl uoroscopically.
c
. Release pressure on the thumb grip of
the handle.
d
. Pull the wire guide pusher’s distal end
back into the fi lter catheter.
Remove the wire guide pusher and fi lter
catheter, leaving the introducer sheath
in place. Reposition the sheath for a fi nal
vena cavogram.
Fig. 9a
Fig. 9c
Fig. 9b
Fig. 9d