




























1-11
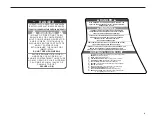
TRAVEL PLAN LOG
The boat listed below should return by:
__________________ ________________ at the latest.
If it has not, please call the emergency numbers
listed at the right.
Police
_________________________________
Coast Guard
_________________________________
Other Authority
_________________________________
Personal
_________________________________
Trip Information
_______________________
_______________________
Departure Date/Time
Departure Location
_______________________
_______________________
Return Date/Time
Return Location
Boat Description
_______________________
_______________________
Boat Name
Type
_______________________
_______________________
Registration Number
Manufacturer
_______________________
Length
_______________________
_______________________
Hull Color
Deck (Color)
_______________________
_______________________
Cabin (Color)
Trim (Color)
____________________________________________________
____________________________________________________
Other Physical Characteristics
Engine
_______________________
_______________________
Type
HP
_______________________
_______________________
Fuel Type
Fuel Capacity
Safety & Emergency Equipment
(YES/NO & NUMBER)
_____________
_____________
______________
Life Jackets
Cushions
Distress Light
_____________
_____________
______________
Flares
Smoke Signals
Flash Light
_____________
_____________
______________
Mirror
Paddles
Anchor
_____________
_____________
______________
Food
Water
Life Raft
Radio
_______________________
_______________________
Onboard (Yes/No)
Type
____________________________________________________
____________________________________________________
Frequencies usually used or monitored
Passenger List
(Use Another Sheet If Necessary)
____________________________________________________
Full Name
_______________________
________________________
Age/Sex
Phone Number
____________________________________________________
Complete Address
____________________________________________________
____________________________________________________
Full Name
_______________________
________________________
Age/Sex
Phone Number
____________________________________________________
Complete Address
____________________________________________________
____________________________________________________
Full Name
_______________________
________________________
Age/Sex
Phone Number
____________________________________________________
Complete Address
____________________________________________________
____________________________________________________
Full Name
_______________________
________________________
Age/Sex
Phone Number
____________________________________________________
Complete Address
____________________________________________________
Time
Date
ALWAYS FILL THIS SHEET OUT COMPLETELY—IN AN EMERGENCY ALL INFORMATION MAY BE HELPFUL
Summary of Contents for 2012 SSi
Page 15: ...1 7...
Page 16: ......
Page 20: ......
Page 49: ...3 14...
Page 74: ...5 16...
Page 75: ...5 17...
Page 93: ......
Page 101: ......
Page 108: ...WIRING SCHEMATICS 12 12 1 196 206 216 SSI...
Page 109: ...12 2 196 206 216 SSI...
Page 110: ...12 3 226 SSI...
Page 111: ...12 4 226 SSI...
Page 112: ...12 5 246 SSI...
Page 113: ...246 SSI 12 6...







































































